I. Introduction
Coronary artery disease (CAD) in firefighters is due to a combination of workplace factors and personal factors such Diabetes mellitus, hypertension, smoking, elevated blood cholesterol (HDL-C), obesity, and a lack of exercise (AHA, 2007). Although not as widely known, firefighters are also exposed to factors in the workplace which are also associated with adverse cardiac outcomes.
II. Cardiovascular effects associated with smoke
Think back to your first fire academy class. You learned that smoke is a combination of heated gases, vapors, and particulate matter. It is also important to remember that the composition of smoke is determined not only by its fuel source, but also by fire conditions such as oxygen availability and temperature (Kulig, 1991). While hundreds of decomposition products can be found, two gases with known cardiovascular effects are carbon monoxide and hydrogen cyanide.
Carbon monoxide (CO)
Carbon monoxide - a product of incomplete combustion - is present in virtually all fire environments. One thing I think many of us are guilty of overlooking is the fact that high CO levels are usually still present during the overhaul phase of an operation and, to make that situation worse, it is during this phase of the operation that many firefighter's remove their self-contained breathing apparatus (SCBA). When CO is inhaled, it disrupts the transport of (and intracellular use of) oxygen which can result in a myocardial injury.
Hydrogen cyanide (HCN)
Hydrogen cyanide is formed due to the incomplete combustion of substances which contain both carbon and nitrogen (e.g. paper, cotton, and wool). It has frequently been detected in residential structure fires in levels that exceed established exposure limits. Like CO, hydrogen cyanide disrupts the intracellular use of oxygen resulting in intracellular hypoxia with cardiac manifestations.
Particulate matter
III. Why are we at higher risk
It is a well-known fact that sleep plays a vital role in helping our body recover from fatigue, illness, and stress. Without it, our metabolic rate begins to decrease resulting in weight gain. A firefighter's "internal biological clock"is often disrupted numerous times during a shift making it difficult to regulate the sleep-wake system. In addition, researcher's at Boston Hospital and Medical Center have determined that prolonged sleep restriction combined with circadian rhythm disruption can be a contributing factor to an increased risk for diabetes.
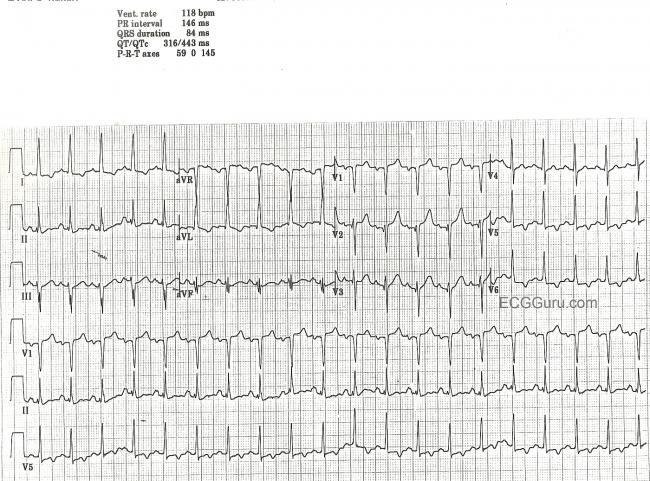 |
| Electrocardiogram (ECG) tracing shows coronary heart disease |
As a firefighter, we are exposed to traumatic stress almost every shift. If we work thirty (30) years that stress will take a toll on our body both physically and mentally. Researchers at the University of California - San Francisco (UC San Francisco) have found that these exposures over the course of a lifetime will experience an increase in inflammation in their body even if they don't develop Post-Traumatic Stress Disorder (PTSD). These increased levels of inflammation also tend to put the person at a greater risk of having an MI. Intervention strategies to combat this stress, such as exercise, yoga, and other health-related activities should be integrated at the start of a firefighter's career.
IV. Conclusion
 |
| Chicago Engine 29 operates at an early morning warehouse fire. |
Additional information: Firefighter deaths from cardiovascular events, Heart disease and firefighters
References
American Heart Association (AHA) [2007]. Risk factors and coronary artery disease. Retrieved on September 19, 2017 from http://www.americanheart.org/presenter.
jhtml?identifier=4726
Hofman, John (September, 2012). Heart disease and firefighters: how and why? Retrieved on September 28, 2017 from http://www.fireengineering.com/articles/2012/09/heart-disease-and-firefighters-how-and-why.html
Hofman, John (September, 2012). Heart disease and firefighters: how and why? Retrieved on September 28, 2017 from http://www.fireengineering.com/articles/2012/09/heart-disease-and-firefighters-how-and-why.html
Kulig, K. [1991]. Cyanide antidotes and fire technology. New Eng J Med 325:1801-1802


